 United Kingdom
United Kingdom
Angel Aligner PRO: Correction of a class II div 1 malocclusion
Dr. Dalia Latkauskiene
Dr. Dalia Latkauskiene
Dr Dalia Latkauskienė received her dental degree in from Kaunas University of Medicine. Since 2002 she has been in full-time private practice. She defended her Phd thesis „Herbst- effects on jaws and dental arches in growing Class II patients“ in 2013.
Dalia Latkauskienė has presented lectures, seminars and continuing education courses on crowned Herbst appliance, mixed dentition treatment, aligner treatment, adult orthodontics, multidisciplinary treatment and combined orhodontic-orthognatic treatment (together with maxillo facial surgon S. Grybauskas DDS, MD, Phd) to dental and orthodontic organizations as well as conferences worldwide.
Current interests focus on orthodontic-orthognatic, non-compliant orthodontic treatment, temporary anchorage devices, adult orthodontics and aligner treatment.
Patient introduction
Age: 25
Gender: Female
Treatment time: 12 months
Number of aligners: 40
Chief complaint: The patient expressed dissatisfaction with the aesthetics of the smile, seeking improvement in alignment and overall appearance. Additionally,the patient reported concerns regarding sensitive teeth, which caused discomfort during daily activities such as eating and drinking. These issues were the primary motivators for pursuing treatment with angel aligner.
Section Class II division 1 malocclusion
Product Pro
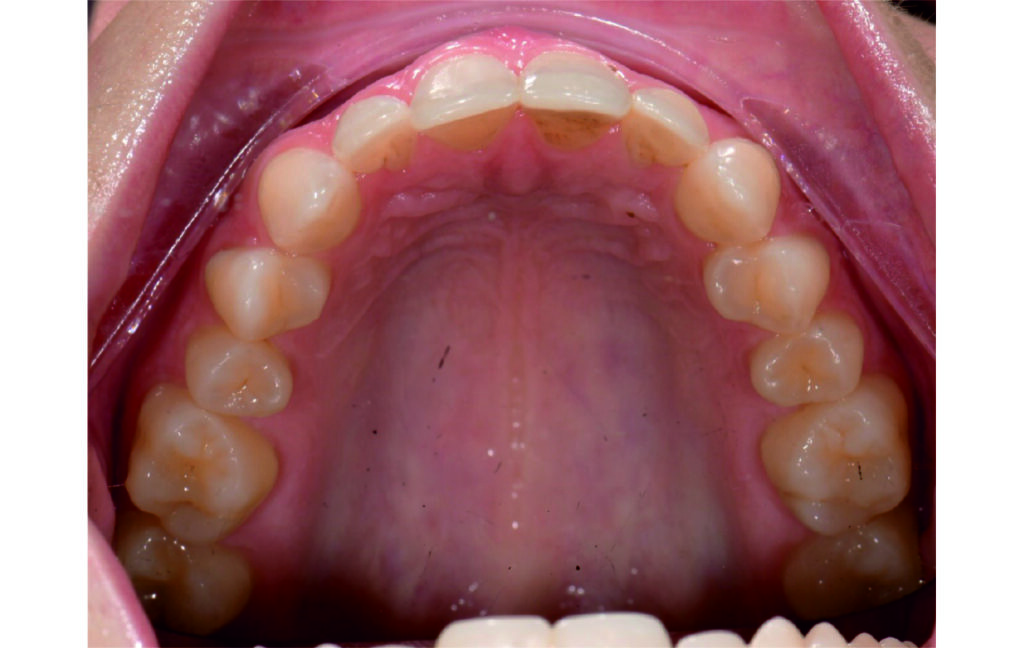
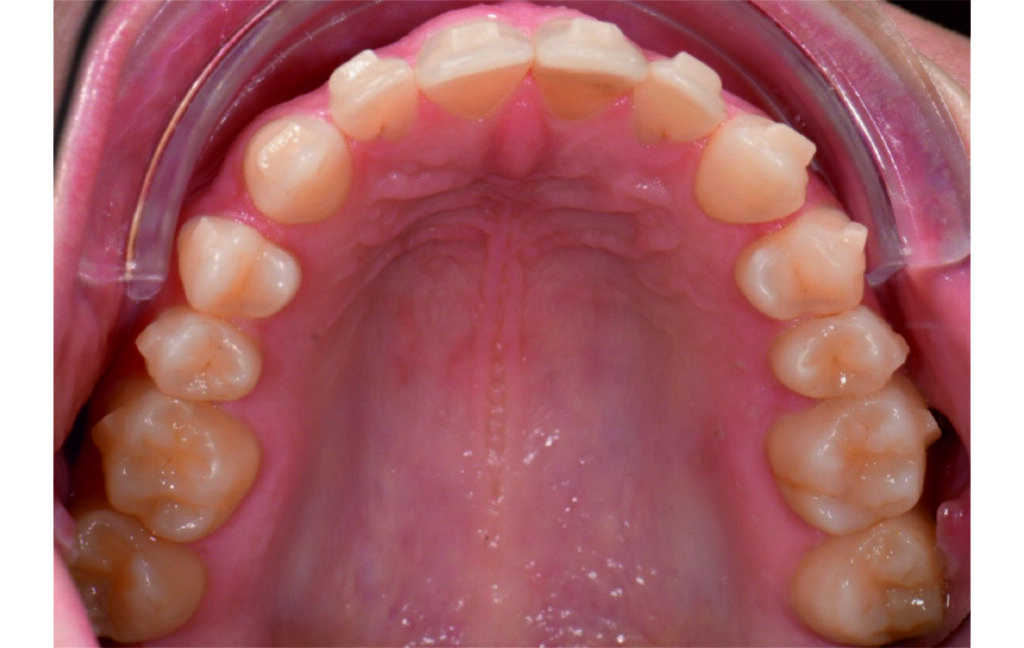
Malocclusion Class II on both sides due to mesial rotation of 16 26
Light mandibular asymmetry to the right with both midline deviation.
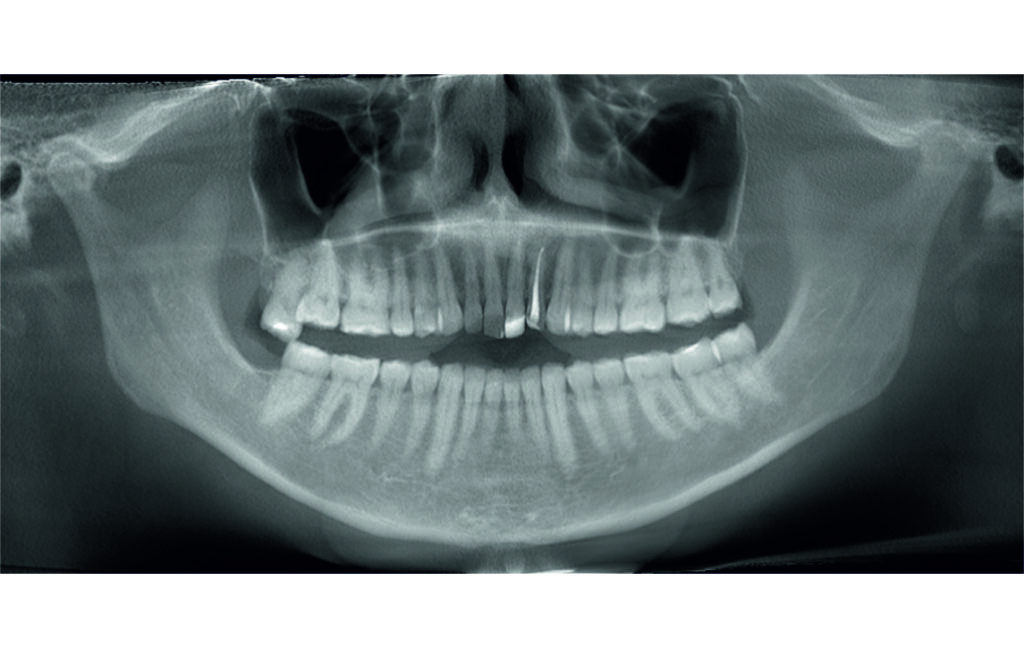
Severe attrition of posterior teeth, night bruxism. Open bite tendency.
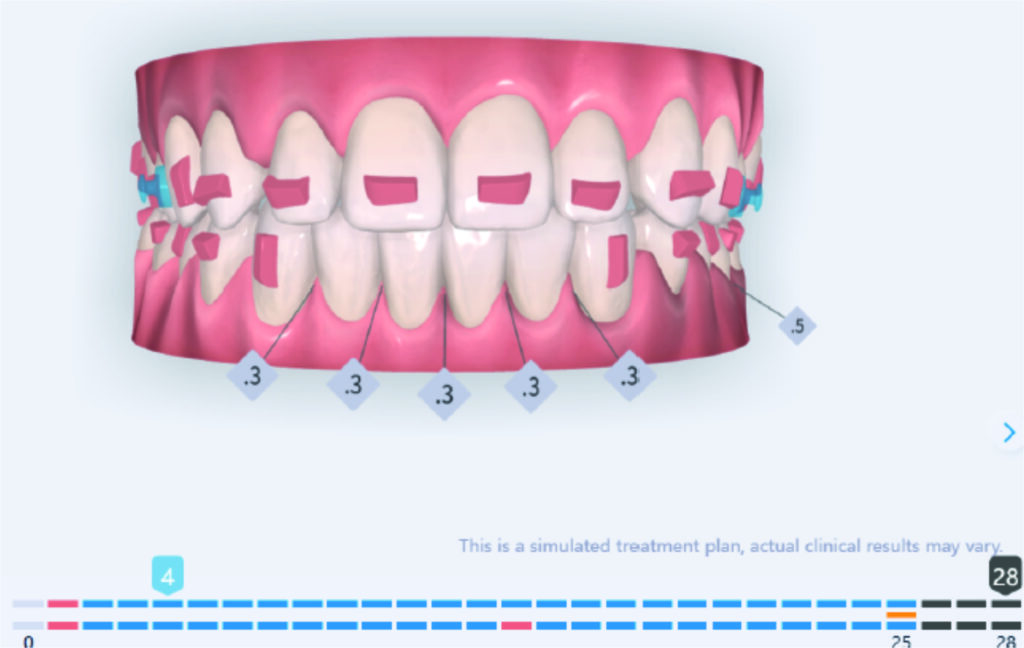
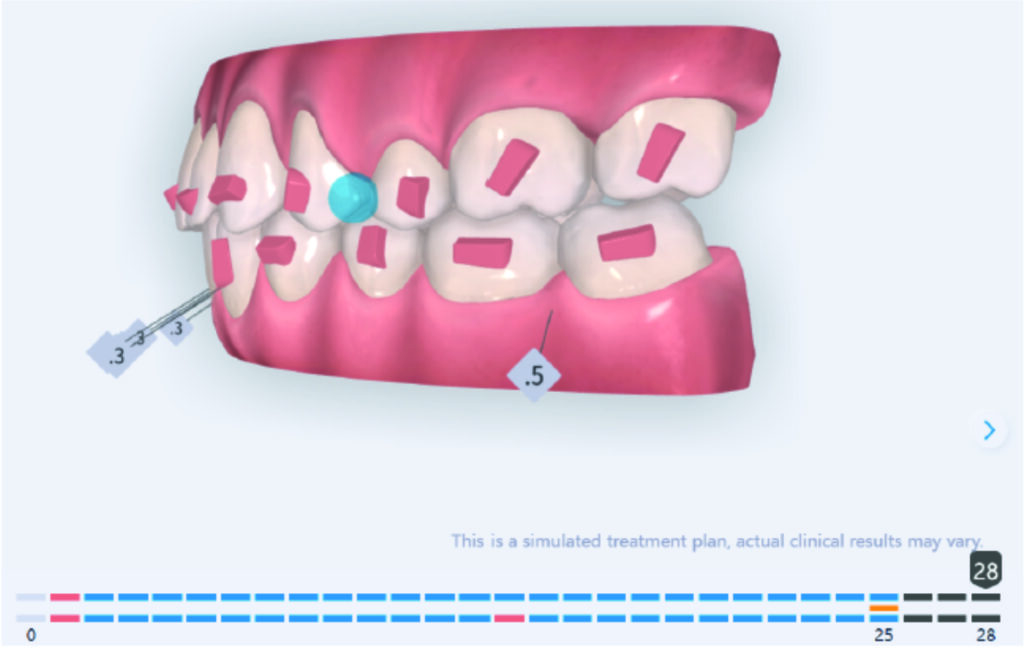
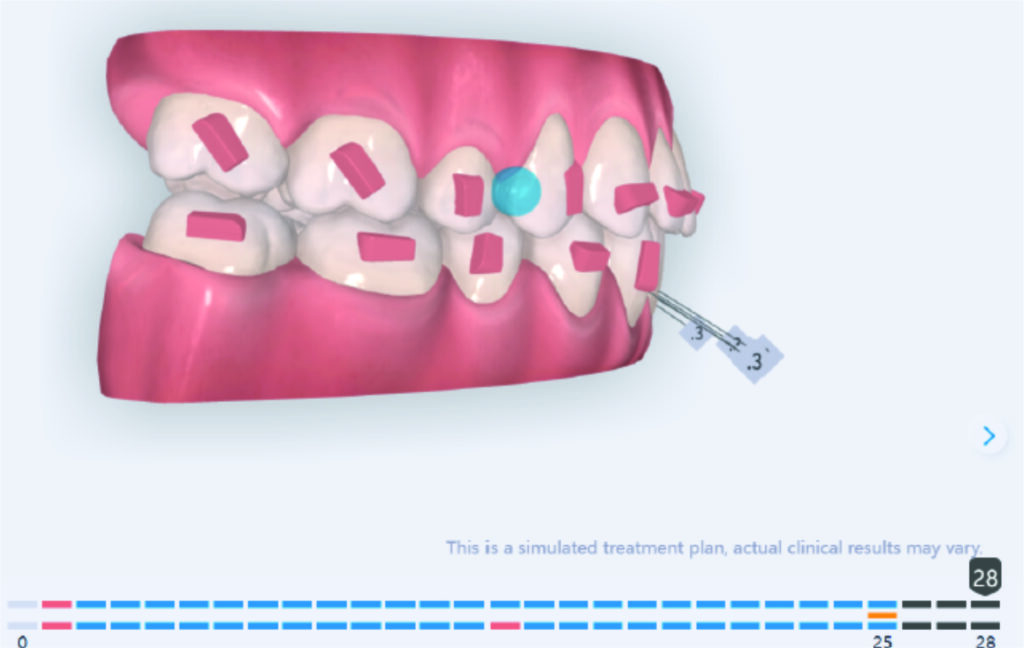
Protocoles and features IPR
Initial Photos and datas







Clinical examination and diagnosis
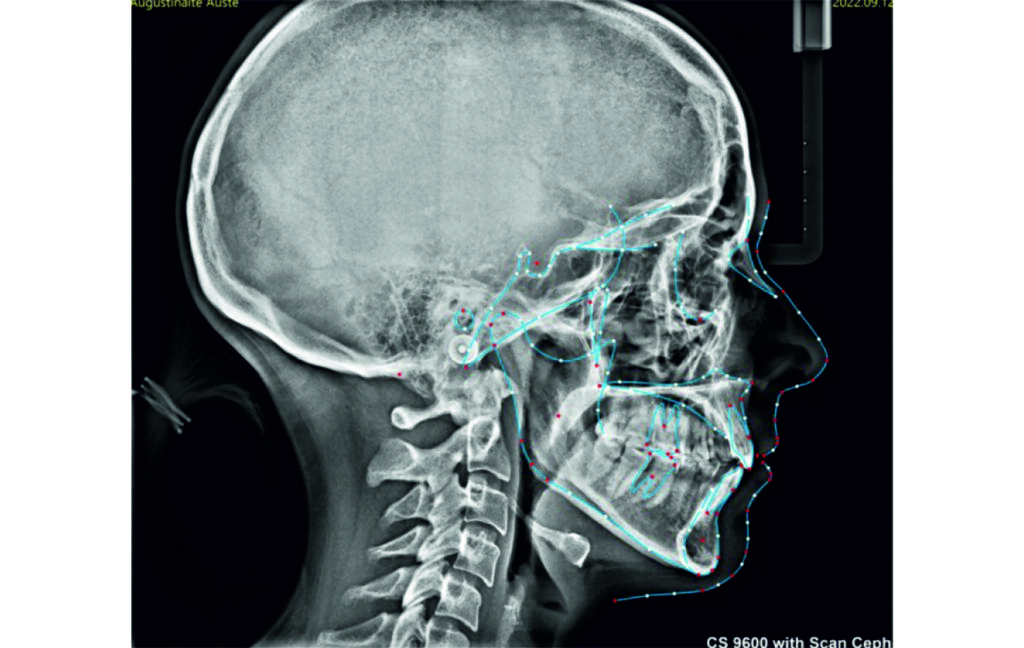
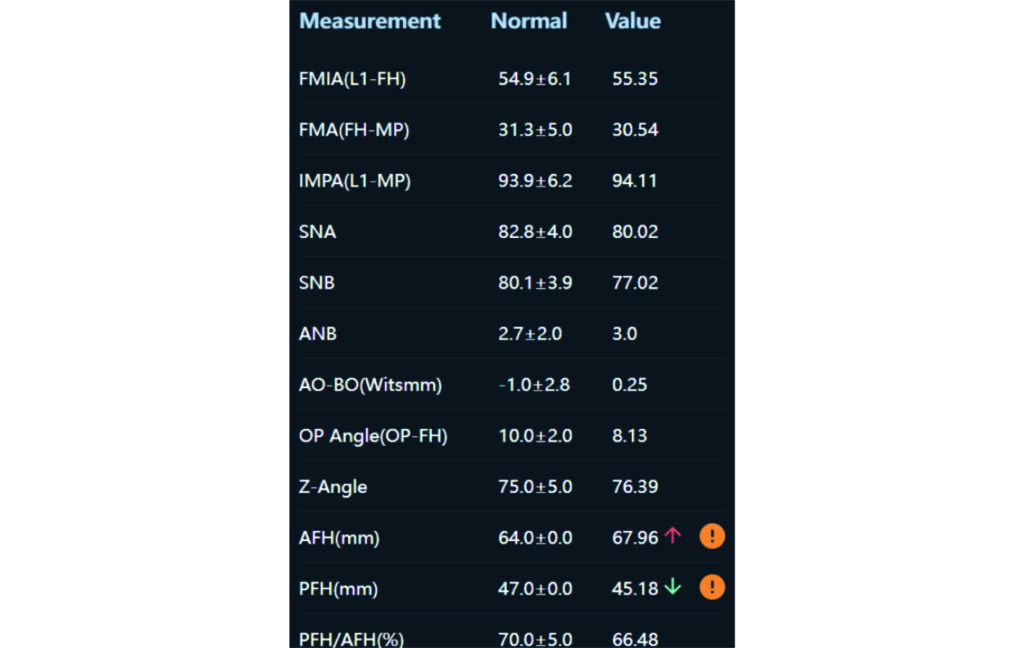
Angle Class II 2mm on the right, Angle Class II 2mm on the left, light mandibular asymmetry to the right, lower central line 1mm to the right, upper central line 1,5mm to the left, 1mm overjet and overbite. Sagittal asymmetry of upper dental arch. Light crowding upper and lower frontal segments, severe attrition of posterior teeth, night bruxism. Normal sagittal position of both jaws, high angle case, steep mandibular ramus,excessive lower facial height, open bite tendency.
Function is normal
Patient Motivation good
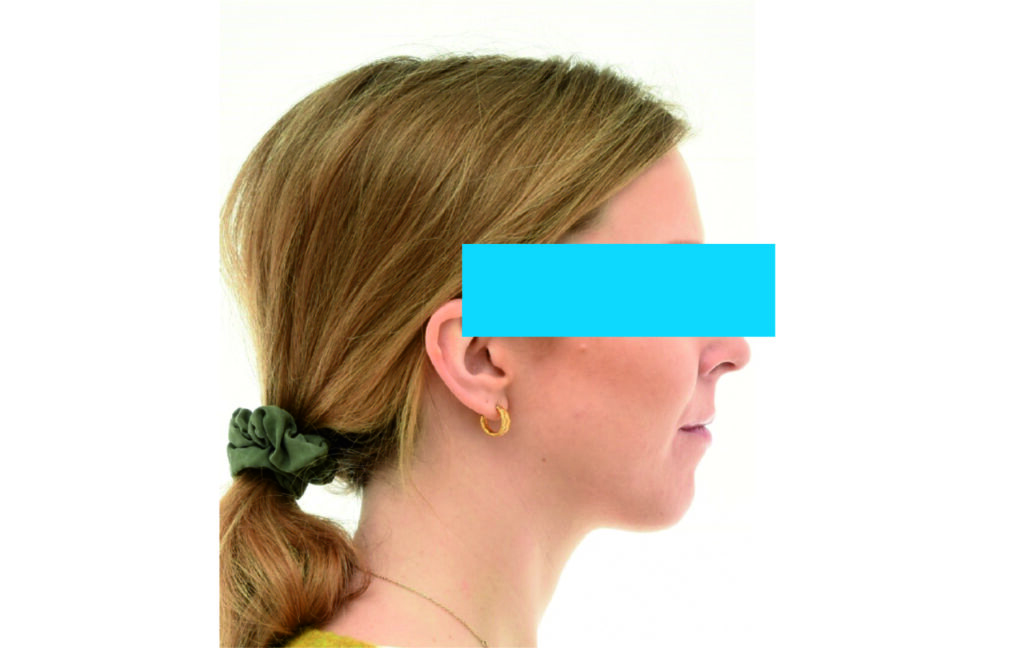
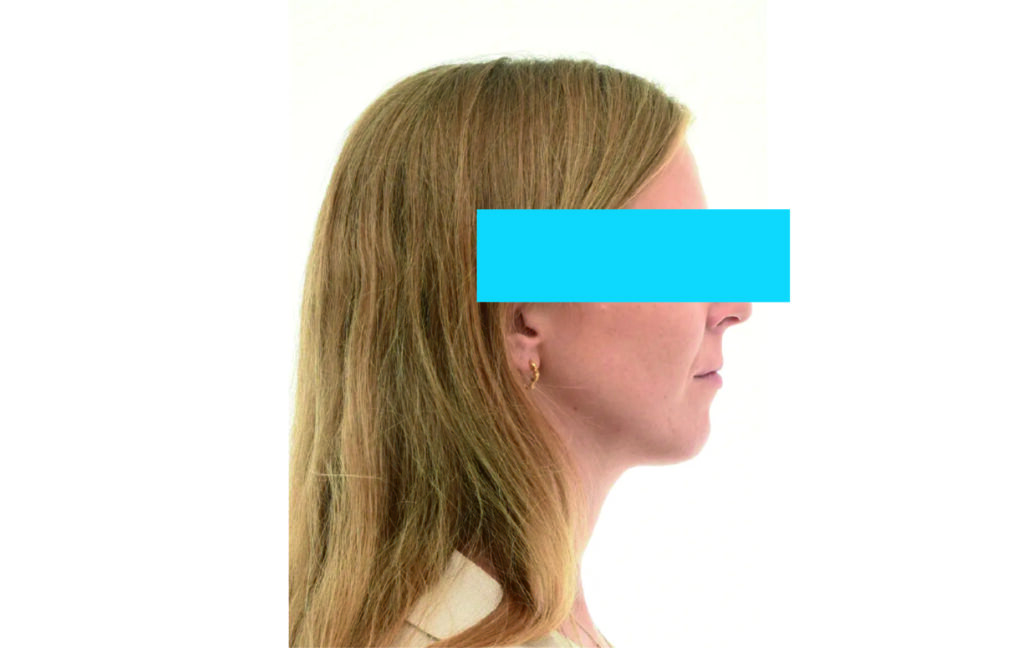
Soft Tissue Analysis: convex profile, lower third of the face increased, slightly retrusive upper and lower lips, lip strain on closure.
Treatment plan
Restore severely damaged teeth via composite restorations
Alignement and expansion 2mm per quadrant.
Distalization in segment 1 to Class I and derotation of 16, move upper central line to fit lower central line.
Derotation 26. IZC anchorage.
Settling the bite in Class I.
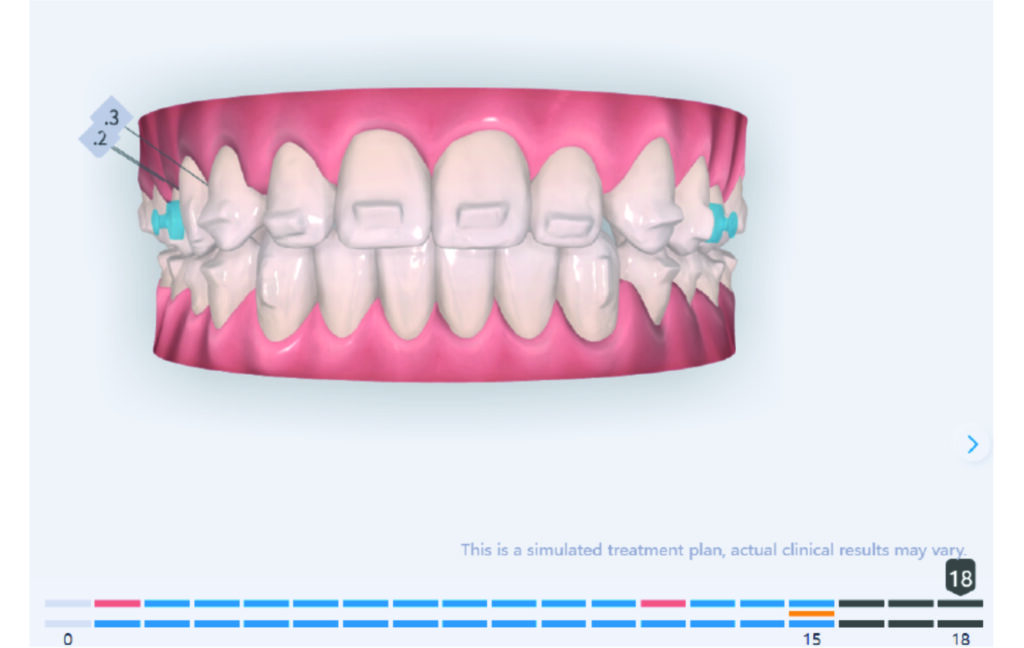
IPR of the lower anterior segment was performed to address Bolton discrepancy.
The case initially presented as a moderate Class II on the right and a Class II tendency on the left, with tapered dental arches and an anterior open bite extending to tooth 26 in segment II.
In segment I, the open bite reached up to the first premolar.
A 1.5 mm deviation of the upper dental midline to the patient’s left was noted, along with a slight mandibular midline shift to the right, likely due to asymmetrical mandibular growth observed in the facial structure. Severe mesial rotations of teeth 16 and 26 were evident in the initial records. As derotation of 16, 26, 17, and 27 progressed up to aligner 16, the premolars in segments I and II moved distally, resulting in a bilateral Class I relationship, as intended in the initial treatment plan.
Treatment details
Derotation of 16 26 allowed Class II correction.
Vertical vector of elastic traction on buttons and IZC helped with the open bite correction.
No sequential distalization for Class II tendency correction was performed due to skeletal anchorage. Lingual attachments were used to improve aligner grip and control tooth movement, as small, angulated lower incisors are difficult to move due to limited anatomy.
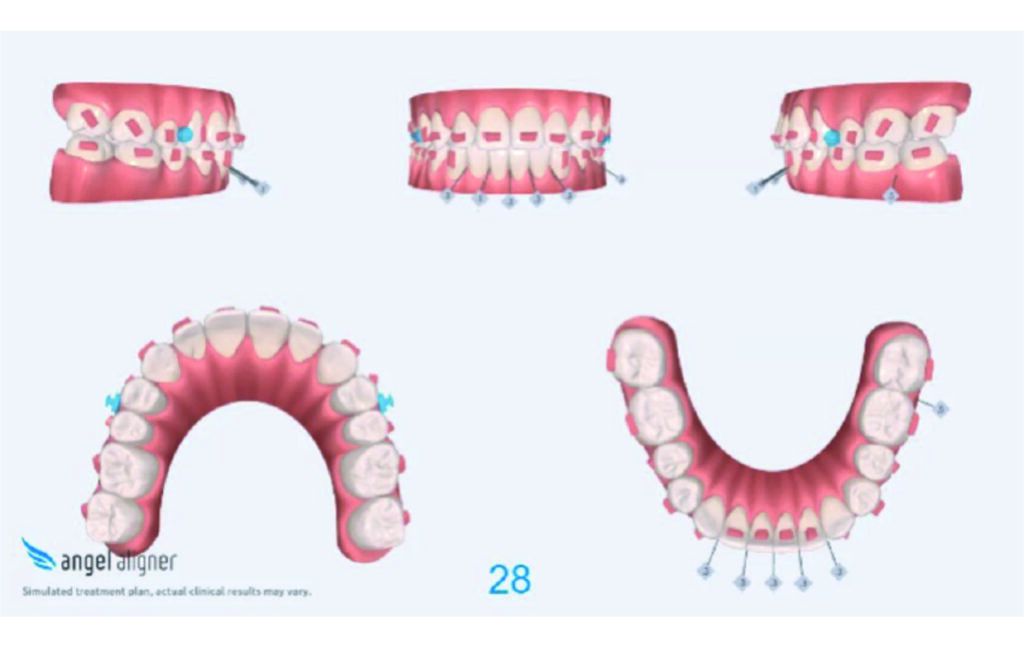
An infrazygomatic crest (IZC) screw with force applied between the upper premolars produces a clockwise rotation of the maxillary occlusal plane. This movement aids in closing the anterior open bite and improves upper incisor display. IZC screws with elastics also enable planned intrusion of the upper molars by 1 mm. Because mandibular derotation after upper posterior correction is difficult to predict, anterior distalization and midline correction were performed in the later stages of treatment.
Treatment setup

Treatment progress










Download the full case to see the treatment results, the conclusion and get more details on the solution
To download this report, you agree to subscribe to the Angel Aligner newsletter. You can unsubscribe at any time in your settings centre.










